Health
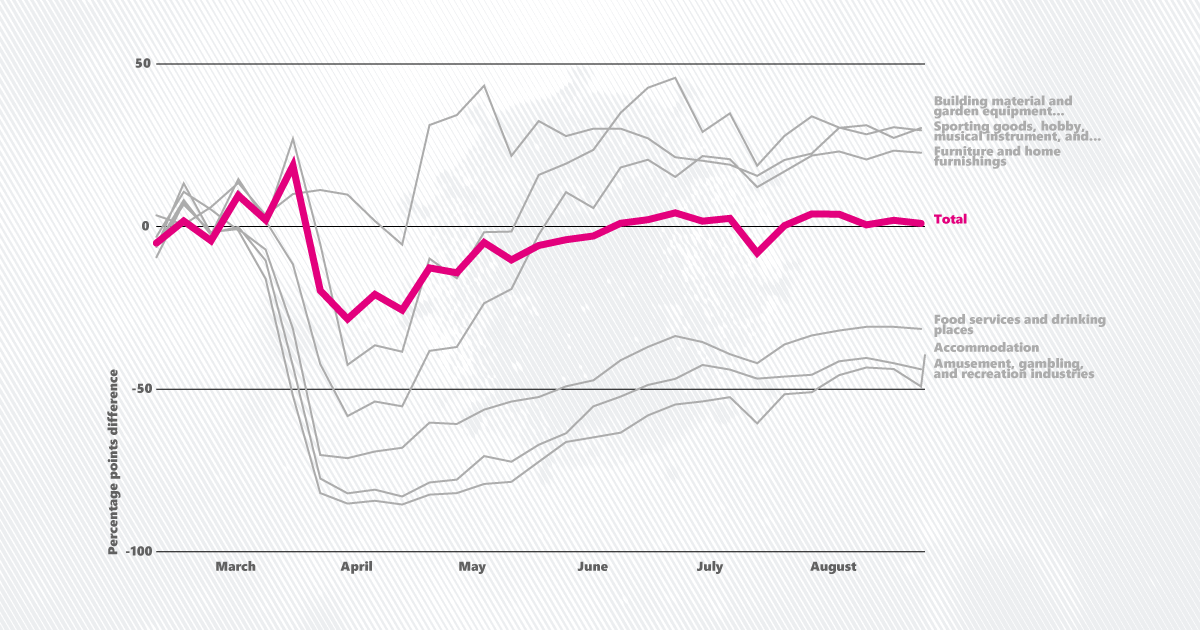
5 things August data says about COVID-19 and the economy
According to the Department of Health and Human Services, most people with mental illness are not violent.[1] Despite this, police officers often end up serving as the first responders to mental health calls, at times resulting in fatal consequences. In 2016, 242 individuals known to have mental illnesses were fatally shot by police, a number that fell to 236 in 2017.
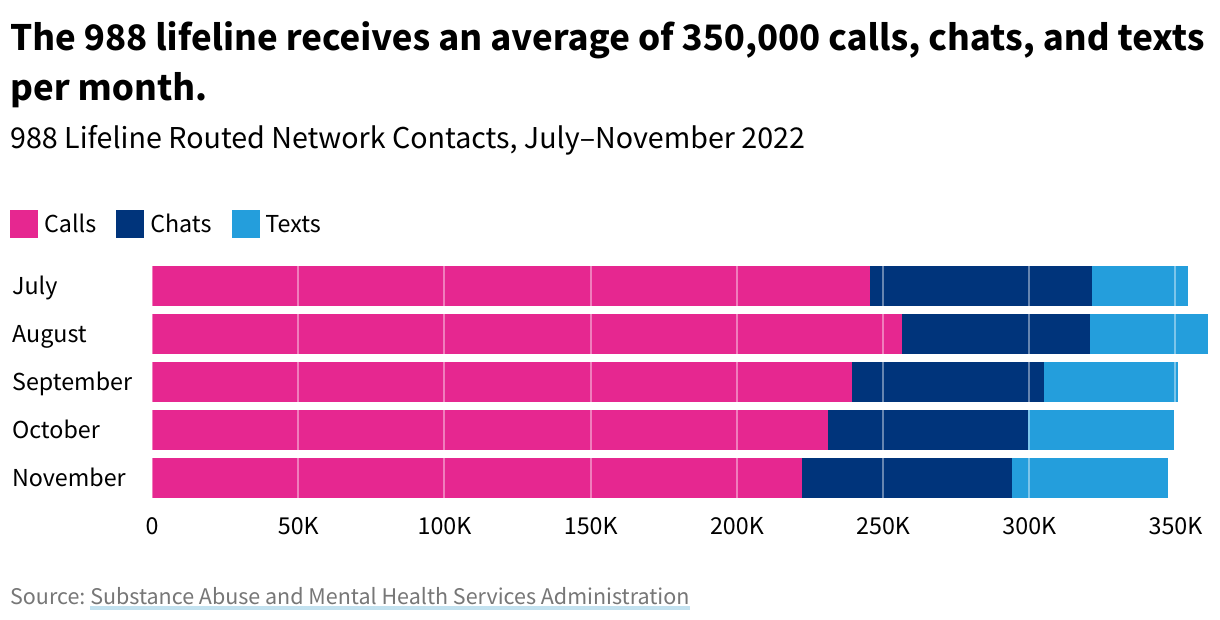
Meanwhile, the country’s demand for professional mental health help is high. According to the Substance Abuse and Mental Health Services Administration, 988, the new national Suicide and Crisis Lifeline, has had an average of 353,000 monthly calls, chats, and texts since its launch in July 2022.
A Department of Justice report points to deinstitutionalization as the single largest contributor to the policing of people with mental health issues.
Deinstitutionalization, or the policy of releasing people with mental illnesses from state mental institutions, began in 1955 with Food and Drug Administration approval of the drug Thorazine. As the first antipsychotic on the market, Thorazine made community-based treatment of mental illness seem attainable.
In the 1960s, a budding advocacy movement and a sequence of class action lawsuits exposed the dire living conditions of institutionalized disabled and mentally ill patients. Federal legislation and public opinion alike began to favor community-based care over institutionalization, and many psychiatric hospitals closed as a result. According to the Congressional Research Service, the number of beds in state and county psychiatric hospitals decreased by over 90% from 1995 to 2005.
As many people with mental illnesses were released from institutions and returned to everyday society, the community-based resources that were meant to help them reintegrate never materialized.
This vacuum in the healthcare system in the health care system caused members of the public to turn to police when they encountered people struggling with mental illness. Police began using arresting and jailing as a short-term solution, which led to a rise in the criminalization and re-institutionalization of people with mental illnesses.
A study cited by the Department of Justice discovered that while in 1955, 0.3% of the US population had mental health issues and was living in a psychiatric institution, in 1999, 0.3% of the population with mental health issues lived in jails or prisons instead.
Today, approximately 10% of all calls to police involve people experiencing a mental health crisis.
Police respond to a wide variety of mental-health related calls. According to one study of Texas law enforcement, the five most common situations that lead to police interactions with people with mental illness are:
Data reveals that, more often than not, people with mental illnesses do not pose a threat to police officers. And yet, research shows that police apply force disproportionately to people with mental illness.
According to an analysis cited by the 2022 report from the Illinois Criminal Justice Information Authority, individuals with untreated mental illness are 16 times more likely than the average civilian to be killed during police contact.
According to another analysis cited by the 2018 US Commission on Civil Rights[2] on police use of force, within the first six months of 2015, police shot and killed a person experiencing a mental health crisis every 36 hours.
Part of the reason for these outcomes may be because many police departments nationwide don’t use de-escalation[3] as standard practice.
A review cited by the Illinois Criminal Justice Information Authority found that only 37% of the police departments in the nation’s 100 largest cities mandated that officers use de-escalation before applying force. Twenty-one departments banned chokeholds and strangleholds.
Law enforcement often does not have adequate training on interacting with someone experiencing a mental health crisis.
The 2018 US Commission on Civil Rights report cited written testimony that law enforcement officers often feel ill-equipped to manage situations involving people with mental illness, partly because they mistakenly perceive their behaviors as “threatening” or “noncompliant.”
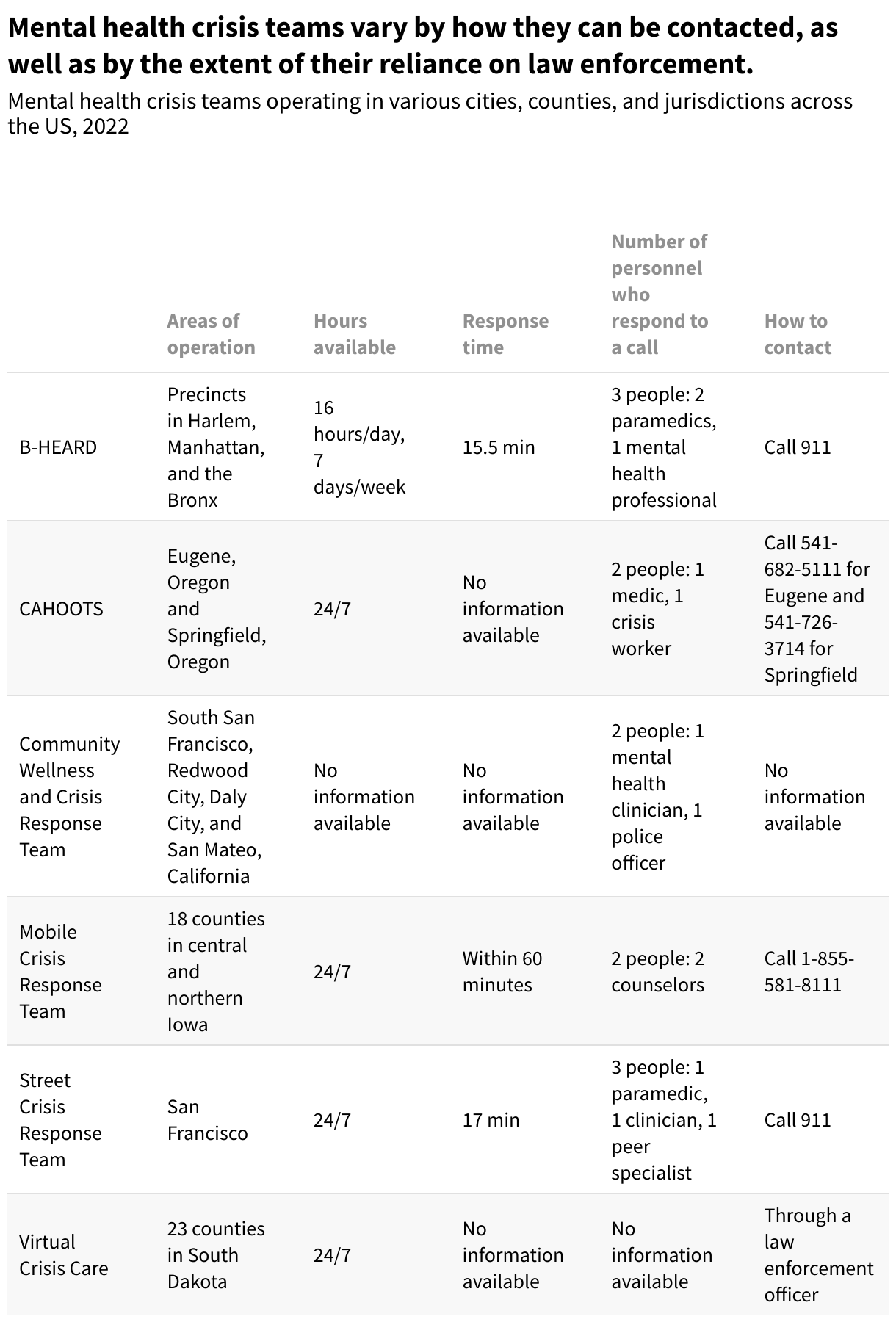
Many behavioral health crises do not require law enforcement intervention. In recognition of this, cities and counties nationwide are funding mobile crisis teams to help reduce instances of police brutality and create a more sustainable way of handling mental health crises. These teams aim to create a safer and more effective method of responding to non-violent mental health situations.
Staffed by paramedics and behavioral health clinicians, mental health crisis teams serve as first responders to people experiencing mental health crises. Many are available 24/7. When called, they often serve as the primary contact for people who are experiencing hallucinations, delusions, suicidal ideation, homelessness, or substance use challenges.
After making contact, the team assesses the client’s condition and tends to their immediate physical and mental health needs. If need be, they transport the patient to medical care.[4] After the initial call, the team follows up with the client to connect them to long-term housing and treatment-related services.
On the city level, mental health crisis teams operate in San Francisco, various cities in San Mateo County, California, various police precincts in New York City, Eugene, Oregon, and Springfield, Oregon. On the county level, they operate in San Diego County, California, 18 counties in central and northern Iowa, and 23 counties in South Dakota.
In South Dakota, the Virtual Crisis Care program provides behavioral health support through iPads, allowing the team to reach many rural areas.
Crisis teams are united in their objectives of decreasing police use of force, reducing the burden on emergency services and systems, and strengthening the public’s awareness of community-based mental health resources.
The Virtual Crisis Care team in South Dakota also includes treating patients in their homes as a measure of success. Involuntarily committing an individual to a psychiatric hospital often proves to be a traumatic experience.
However, crisis care teams vary widely in the extent of their reliance on law enforcement during crisis calls. The Street Crisis Response Team in San Francisco only uses law enforcement as a last resort, but the Community Wellness and Crisis Response Team in San Mateo County, California, makes it a standard practice to pair a mental health clinician with a police officer.
The crisis teams also vary in the mode by which they can be contacted. For example, while anyone in Eugene can use a hotline to call a CAHOOTS team, only law enforcement can call South Dakota’s teams.
The Eugene Police Department estimates that CAHOOTS diverts between 3% and 8% of calls from city police every year.
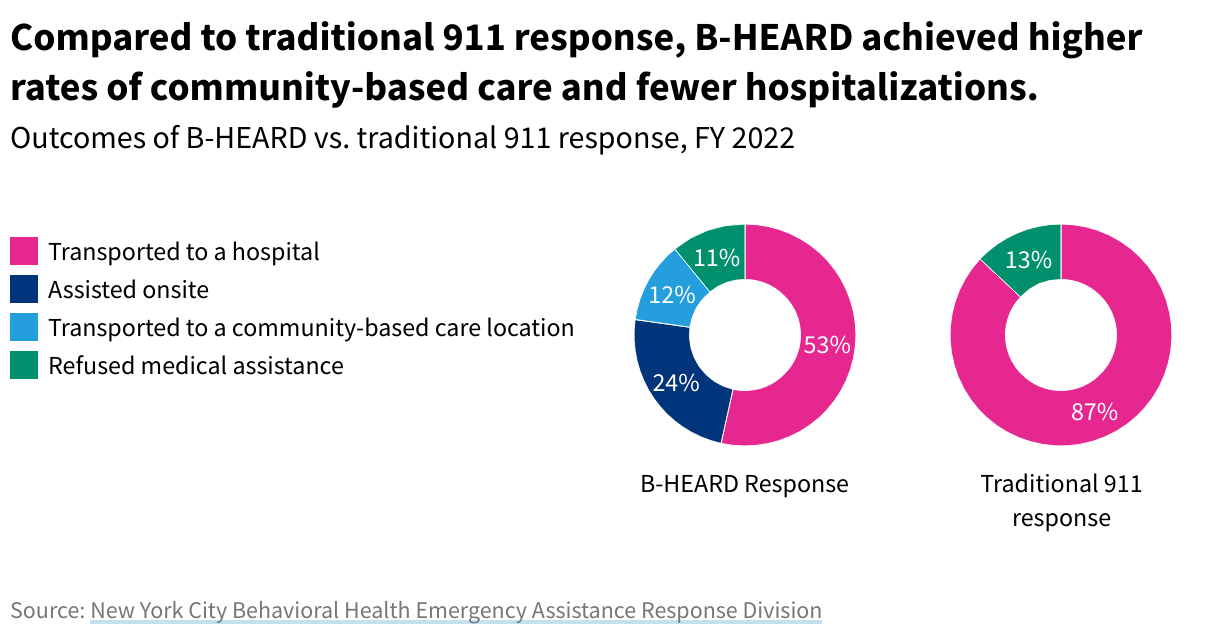
In New York, the establishment of the Behavioral Health Emergency Assistance Response Division (B-HEARD) has resulted in fewer hospitalizations and higher rates of community-based care. When compared to the outcomes of traditional 911 response during 2022, B-HEARD yielded significantly lower rates of hospitalization: 87% of people served by traditional 911 were transported to a hospital, compared to B-HEARD's 54%.
Plus, 36% of those treated by B-HEARD were treated within their community: 24% were treated onsite, while 12% were transported to community-based mental health clinics,[5] such as the East Harlem Support and Connection Center.
Outcomes of B-HEARD vs. traditional 911 response, FY 2022
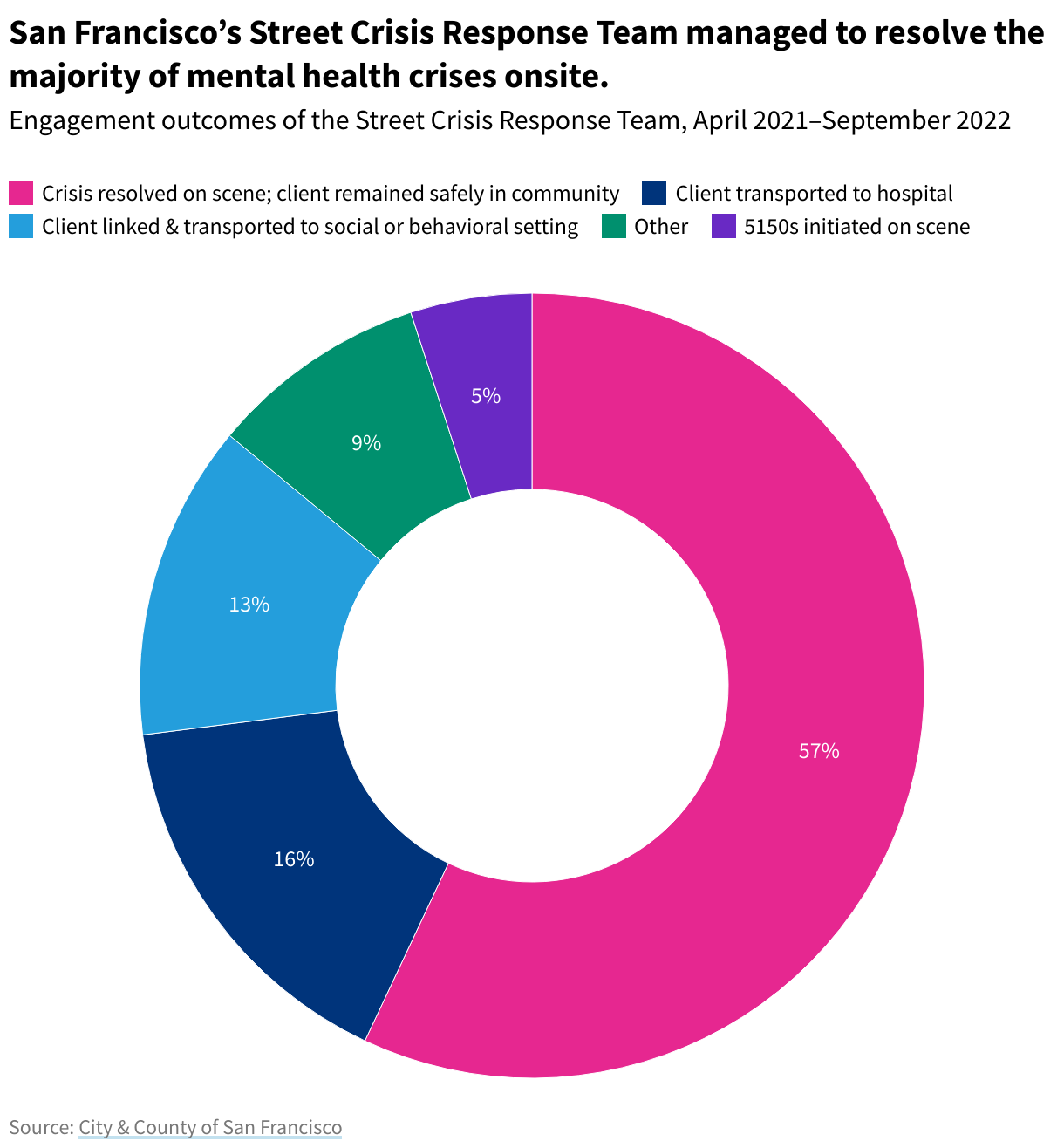
Similarly, San Francisco’s Street Crisis Response Team has been able to resolve 57% of the crises it was called to onsite without removing their patient from their community.
Five percent of crises the Street Crisis Response Team resolved resulted in 5150s. A 5150 is the section of California law that allows someone experiencing a mental health crisis to be involuntarily held in a psychiatric hospital for up to 72 hours.
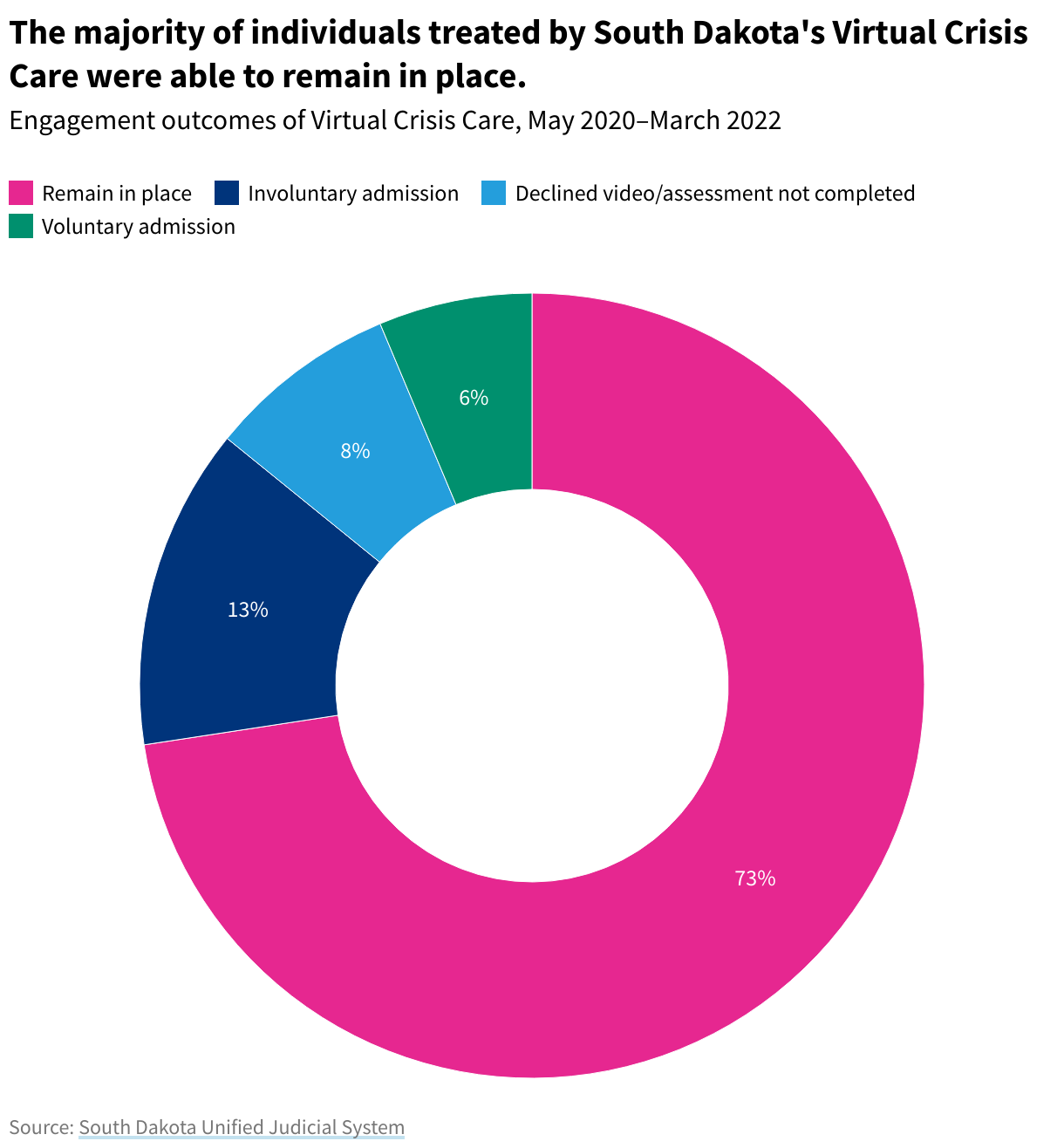
Finally, the Virtual Crisis Care program, which measures success by the number of involuntary admissions to psychiatric hospitals that have been diverted, diverted 79% of its patients from 2020 to 2022. Instead, those patients were treated at home or checked into a mental health institution.
More than half of the mental health crisis teams mentioned above are pilot programs, meaning that they currently lack permanent sources of funding. City and county governments will evaluate the results and associated costs of the crisis teams to determine whether they will continue.
If you or someone you know is struggling with mental health, the 988 Suicide & Crisis Lifeline offers 24/7 free and confidential support.
For a fuller picture of health in the US, read about mental health care access in the US and the risk of suicide for the young, LGTBQ and Native Americans. Get the data directly in your inbox by signing up for our weekly newsletter.
The small fraction of people with mental illnesses who exhibit violent behavior do so when they are actively experiencing psychosis, especially when their symptoms are exacerbated by drug and alcohol abuse, co-occurring disorders, and failure to take medication. While people with severe mental illness commit between 3% to 5% of violent acts, people with severe mental illness are 10 times more likely to be victims of violent crime than the average person.
While national data on police use of force is inadequate, this is one of the most recent government reports issued on the subject.
De-escalation is defined as “Decreasing the emotional, mental, and physical stress levels of an individual or situation using non-verbal and verbal de-escalation techniques.”
Mental health crisis teams do not themselves keep or detain individuals. If they are not able to assist an individual onsite, they transport them to a community mental health clinic, or as a last result, a psychiatric hospital.
As opposed to psychiatric institutions, in which individuals can be committed for long periods of time, local health clinics are meant to provide a sustainable way of providing care to individuals within their communities, without removing them from their homes.




